Due to the complexity of depression, there is no single pathological mechanism that can fully explain the cause of depression in every individual patient. However, the antidepressants developed in the past 30 years only targeted the monoaminergic system and failed to take other possible pathological causes into account. Many depression patients failed to achieve remission with antidepressant treatment in the past.
Currently, the medical community is actively developing new antidepressant drugs that target other systems, including the glutamate system. Through establishing a dual-MoA strategy, it is possible for patients to relieve symptoms in a shorter period of time.
In the past few decades, the monoamine hypothesis proposes that MOD patients have depleted concentrations of serotonin, norepinephrine, and dopamine. Currently in the market, most of the oral antidepressants act based on the monoaminergic system, and improve the patient's condition through increasing the monoamine level.
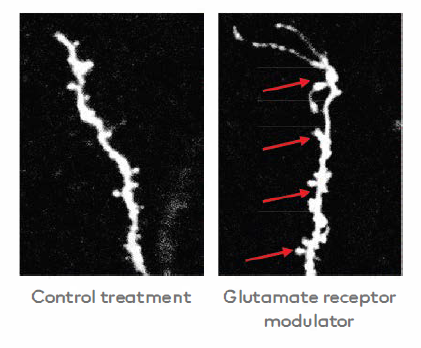
Glutamate is the main excitatory neurotransmitter in the central nervous system and plays an important role in more than half of the neuronal connections in the brain. In recent years, studies have found that the abnormal transmission of glutamate signals in patients with depression reduces the amount and strength of brain connections between neurons in some key regions of the brain, which in turn affects emotional control.
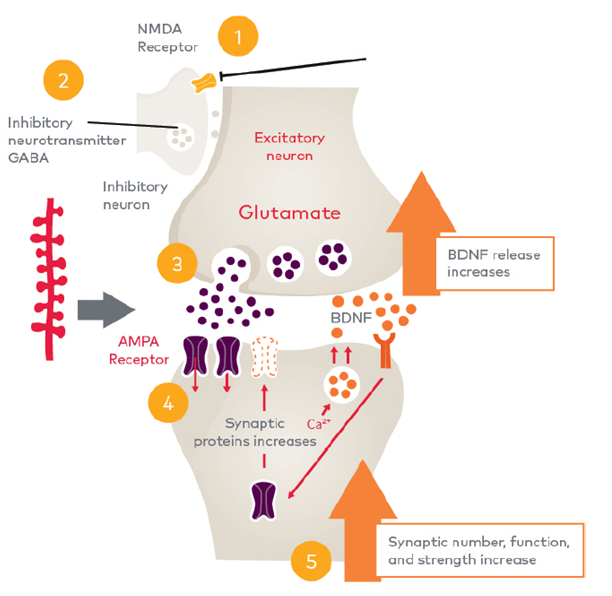
- Esketamine nasal spray binds to and inhibits the NMDA receptor
- This prevents the release of the chemical messenger GABA, which originally interrupted glutamate release
- A surge of glutamate releases into the synaptic cleft
- The stimulation of AMPA receptors triggers a number of intracellular processes, resulting in the release of protein factors that encourage synaptic growth
- As a result, synapses could be restored with increased activity and strength


Esketamine nasal spray is self-administered by patient under supervision by healthcare provider. Each device delivers a total of 28 mg, in two sprays (one per nostril). For the first 4 weeks, patients need to take it twice a week. For the next 4 weeks, patients would need to take it once a week. Thereafter, patients can take it once a week or every two weeks. If necessary, the doctor can reduce or increase the dose at each course of treatment according to the patient's condition to maintain the response to treatment.
































