Facial pain is a relatively common clinical condition with multiple aetiologies, often requiring the expertise of various medical specialists.
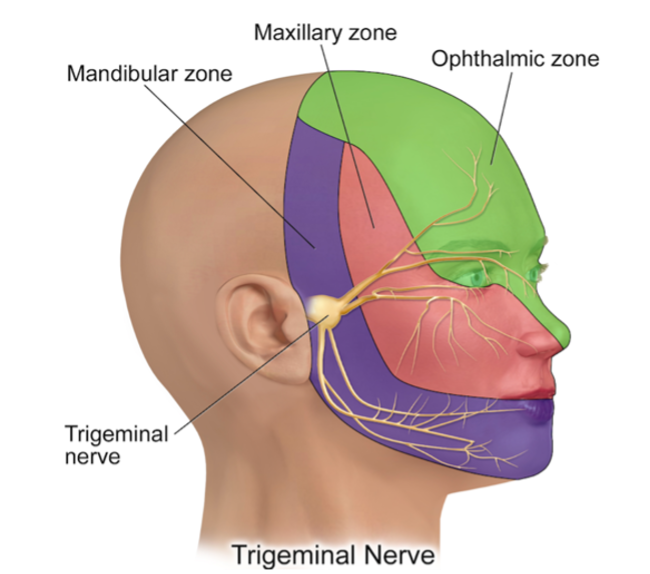
The sensory functions of the face are primarily managed by the trigeminal nerve, which has three branches responsible for transmitting pain sensations from the forehead, maxilla, and mandible. In addition to superficial sensations, the trigeminal nerve also conveys deep sensations from structures such as the sinuses, gums, tongue, and even the intracranial meninges. Due to the complex structure of cranial nerves, there are many potential causes of facial pain. Common conditions include herpes zoster outbreaks, postherpetic neuralgia, trigeminal neuralgia, dental pain, and temporomandibular joint disorders. Severe intracranial tumours or vascular diseases can also lead to facial pain. Diagnosis often requires a detailed medical history and clinical examination, alongside imaging studies, as it involves multiple specialties, including oral and maxillofacial surgery, dentistry, otolaryngology, and neurology.
Clinical Presentation of Trigeminal Neuralgia
Trigeminal neuralgia is a type of facial pain characterised by sudden, severe pain on one side of the face, described as sharp, stabbing, or electric shock-like. The pain typically lasts from a few seconds to 1-2 minutes and often occurs in areas such as the upper lip, nostrils, corners of the mouth, gums, and buccal mucosa. Triggers can include touching the face, eating, or brushing teeth. The recurrent nature of these pain episodes can severely impact the patient's quality of life and mental well-being.
Aetiology of Trigeminal Neuralgia
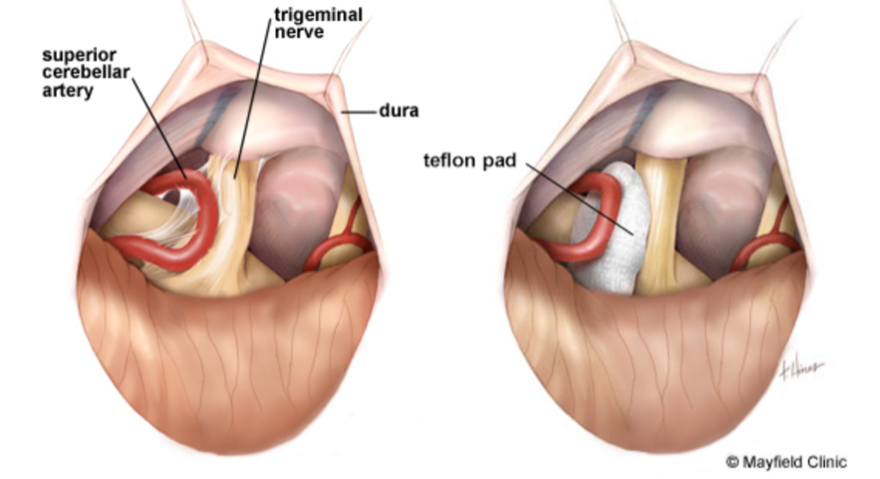
Primary trigeminal neuralgia is primarily caused by the compression of the trigeminal nerve root as it exits the brainstem, usually by abnormally positioned blood vessels, such as the cerebellar artery or vein. This compression can create indentations on the trigeminal nerve root, leading to localised thinning and damage of the nerve sheath, resulting in short-circuiting between nerve fibres and causing trigeminal neuralgia.
Diagnosis
The diagnosis of trigeminal neuralgia is based on typical neuralgic symptoms, the exclusion of secondary factors, and the use of imaging studies. Magnetic resonance imaging (MRI) can help rule out intracranial structural lesions and assess the degree of vascular compression on the nerve.